

With NYC plan for mentally ill, hospitals face complex task
New York City’s latest plan to keep mentally ill people from languishing in public is billed as a common-sense strategy to get them help.
By encouraging police officers and city medics to take more psychologically disturbed people to hospitals, even if they refuse care, Mayor Eric Adams says he’s humanely tackling a problem instead of looking away. But his policy will have to navigate a legal challenge and a cool reception from some city lawmakers. In emergency rooms, psychiatrists must determine whether such patients need hospitalization, perhaps against their will.
It’s no simple decision.
“Some people come in and they are very agitated, and they need to be restrained as soon as they walk into the emergency room. … But there are also people who come in and they’re very calm and quiet, but they just tried to kill themselves two hours ago,” says Dr. Joel A. Idowu, who chairs the psychiatry department at Richmond University Medical Center on Staten Island.
“A person who’s stable now might become unstable tomorrow,” he said.
Adams, a police captain-turned-politician, announced the plan in late November. The first-term Democrat has focused on what he views as restoring a sense of safety and civic functionality disrupted during the coronavirus pandemic. Among other things, less crowded streets and subways brought new visibility to the people living on them, some of them mentally ill.
Under state law, police can compel people to be taken to hospitals for evaluation if they appear to be mentally ill and their behavior poses a substantial risk of physical harm to others or themselves.
That’s often interpreted to mean people who are violent or suicidal. But Adams said he’s using room within the law to address people “whose illness is endangering them by preventing them from meeting their basic human needs.”
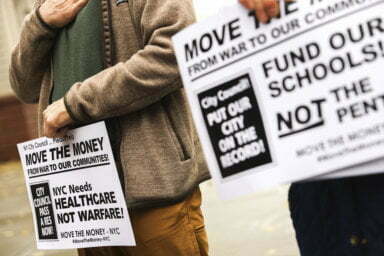
The mayor cites “a moral obligation to help them get the treatment and care they need,” but civil liberties organizations and mental health advocacy groups decry his response as draconian, blinkered and legally suspect. Critics rallied outside City Hall this week and have asked a federal judge to halt the policy; a hearing is scheduled Monday.

It comes amid efforts around the U.S. to separate mental health treatment from law enforcement, including the new nationwide 988 mental health emergency hotline and moves in New York and other cities to handle at least some crisis calls with behavioral health professionals instead of police.
“We need to make mental health care like medical care, a health issue responded to and treated by the people with the right training, at the right time, in the right places,’’ said American Psychiatric Association President Dr. Rebecca Brendel. She maintains that using law enforcement authorities to respond to mental health crises unfairly criminalizes the mentally ill.
Adams said officers will have access to real-time input from mental health professionals and will strive to persuade people to accept help voluntarily. His administration has stressed that while police can send someone to a hospital, it’s up to doctors whether the person needs to stay there or can be safely released for outpatient care.
The complexity, and stakes, became tragically clear when a Rochester, New York, family called 911 in March 2020 about a loved one who was behaving erratically and saying he wanted to die. Once at a hospital, Daniel Prude calmly and appropriately answered questions and said he wasn’t suicidal or homicidal, according to a psychiatrist’s grand jury testimony. The hospital released him.
Hours later, police found Prude running in Rochester’s snowy streets. Officers eventually held him down until he stopped breathing; he was taken off life support days later.
In general, when a patient arrives for emergency psychiatric evaluation, the first step is to ascertain whether a medical problem or drug use is causing the person’s behavior. If not, psychiatrists assess the patient partly by observing and asking questions. But they also seek information from loved ones, prior mental health providers and anyone else who can shed light.
“You can’t just go with what you see or what the patient has told the nurse,” because the person may be unable or unwilling to give a complete picture, says Dr. Madhu Rajanna, the interim chief of psychiatry at St. John’s Episcopal Hospital on New York City’s Rockaway Peninsula.
Staffers might need to calm combative patients — St. John’s says it doesn’t use restraints for that purpose and rarely employs sedatives — or discern whether cooperative patients who insist they’re feeling better are truly well enough to leave.
St. John’s emergency room usually is evaluating eight to 10 psychiatric patients at any given time, and each is supposed to be either admitted or released within 24 hours. (Some other hospitals can hold people for 72 hours for observation in specialized psychiatric emergency programs.)
Rajanna and emergency medicine chair Dr. Leigha Clarkson said St. John’s 43 adult psychiatric beds are generally sufficient, though the hospital tries to release people swiftly once it’s safe.
Citywide, however, Adams’ new policy could test capacity after hundreds of psychiatric beds were converted for COVID-19 cases. The state recently pledged 50 new psychiatric beds, and Adams promised “to find a bed for everyone that needs” one.
It’s possible many people won’t. Richmond University Medical Center’s psychiatric emergency program, for instance, discharges about 3/4 of patients after assessment, Idowu said.
Deciding whether patients stay or go “can be anxiety-provoking sometimes. Because it’s not perfect,” he said, but the goal is that “you don’t leave anything to chance.”